

美国国家压疮咨询委员会(National Pressure Ulcer Advisory Panel ,NPUAP)2016年4月13日公布了一项术语更改声明:将“压力溃疡”(Pressure ulcer)更改为“压力损伤”(Pressure injury),并且更新了压力性损伤的阶段划分系统。
在NPUAP公布的压力性损伤阶段划分系统中,“压力性损伤”替代了“压力性溃疡”。这一更改更加准确地描述了完整或溃疡皮肤处的压力性损伤。在之前的阶段划分系统中,1期和深部组织损伤期用来描述完整的损伤皮肤,其余阶段划分描述开放性溃疡皮肤。由于所有的阶段划分都将损伤纳入了“压力性溃疡”的范畴,这导致了一些混淆。除了术语的改变,新的压力损伤阶段划分系统中,阿拉伯数字替代了罗马数字,“可疑深部组织损伤”名称中去除了“可疑”二字。另外还增加了“医疗器械相关性压力性损伤”以及“粘膜压力损伤”两个定义。
压力损伤:
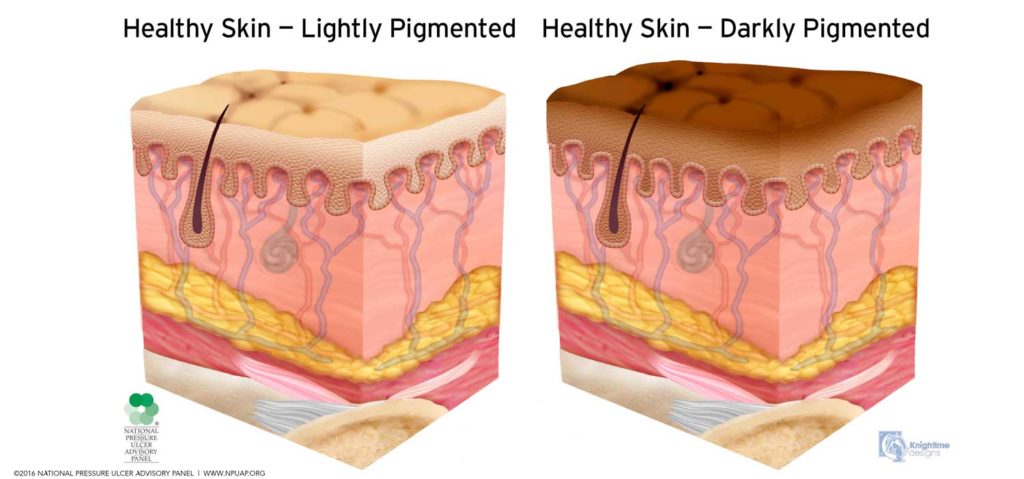
压力损伤通常是在骨突出处与医疗或其他设备对皮肤和皮下软组织的局部损伤。可以表现为完整的皮肤或开放性溃疡并且可能伴有疼痛。压力损伤是由于强烈和(或)长期的压力或压力联合剪切力导致。软组织对压力和剪切力的耐受性可能会受到微环境、营养、灌注、合并症和软组织情况的影响。
第1阶段压力损伤:皮肤完整,指压后不变白的红斑
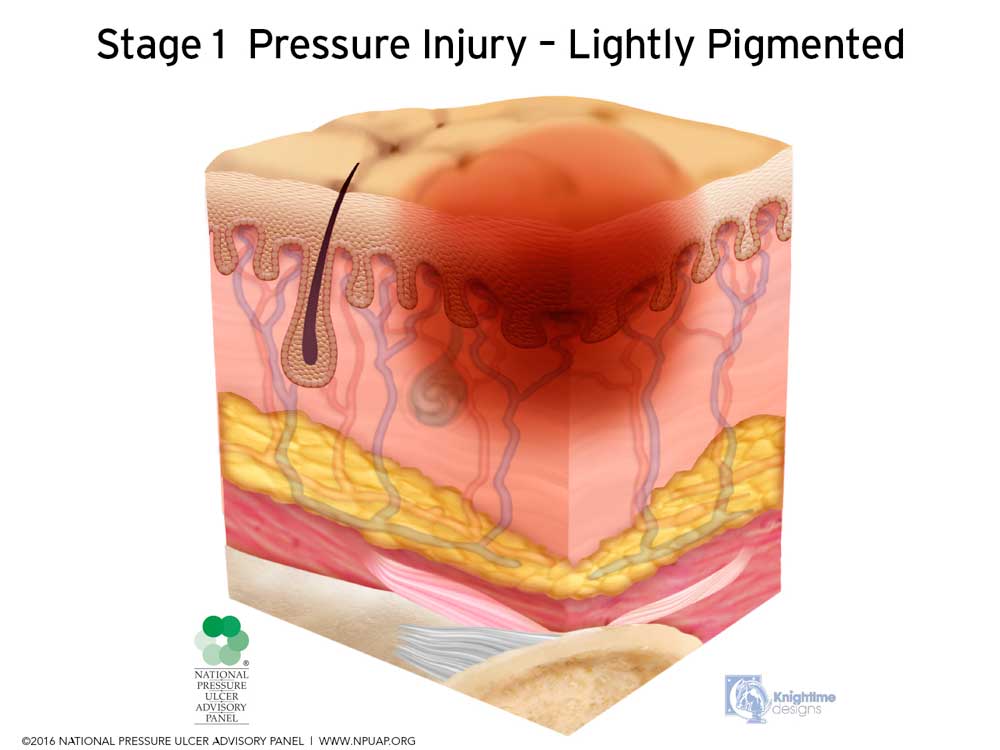
第1阶段压力损伤-轻度色素沉着 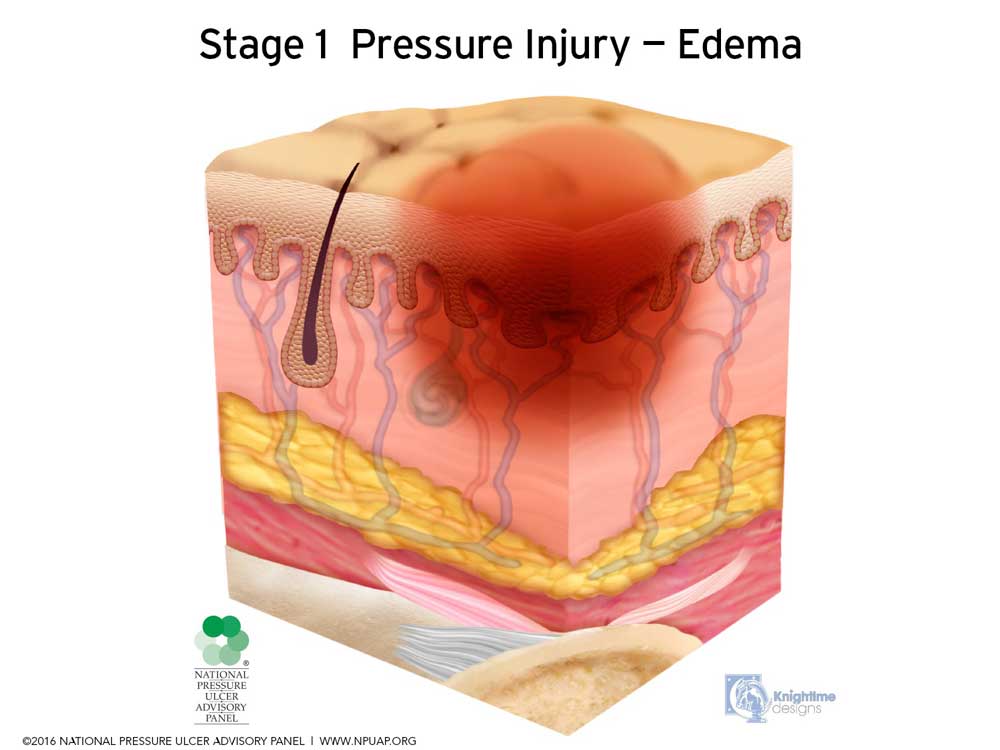
第1阶段压力损伤-水肿 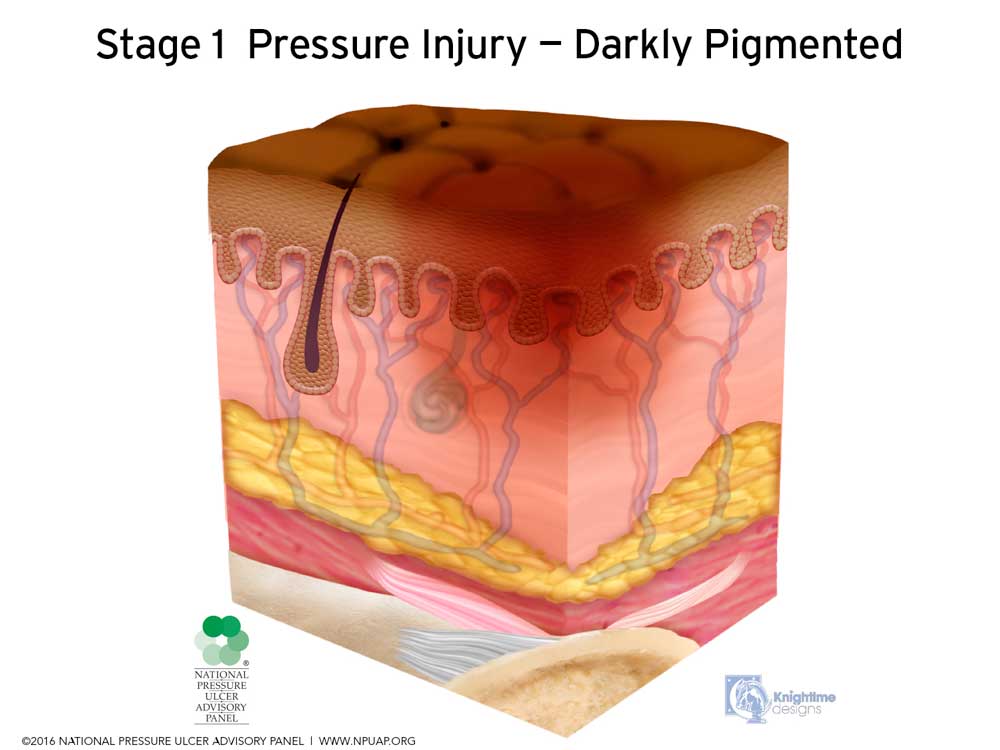
第1阶段压力损伤-颜色较深 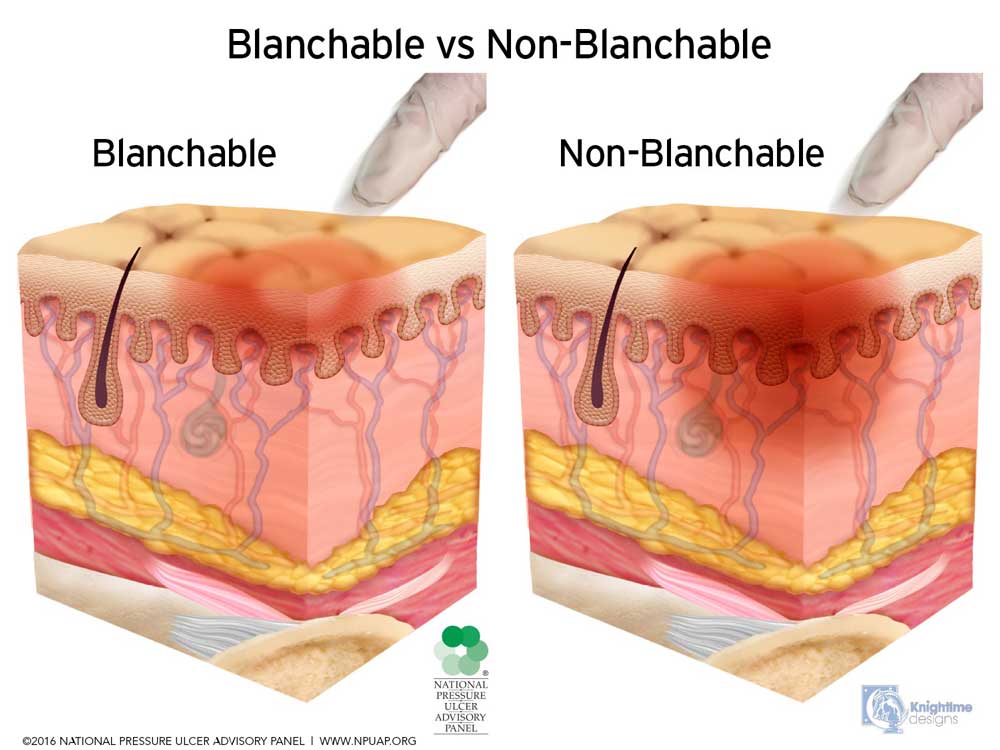
指压时红色消失状态对比
局部皮肤完好,手指按压后不变白的红斑,在深色皮肤中表现可能不同;指压变白红斑或者感觉、皮温、紧致度的改变可能比观察到皮肤改变更先出现。此期的颜色改变不包括紫色或栗色变化,因为这些可能表明存在深部组织压力损伤。
第2阶段压力损伤:真皮层暴露
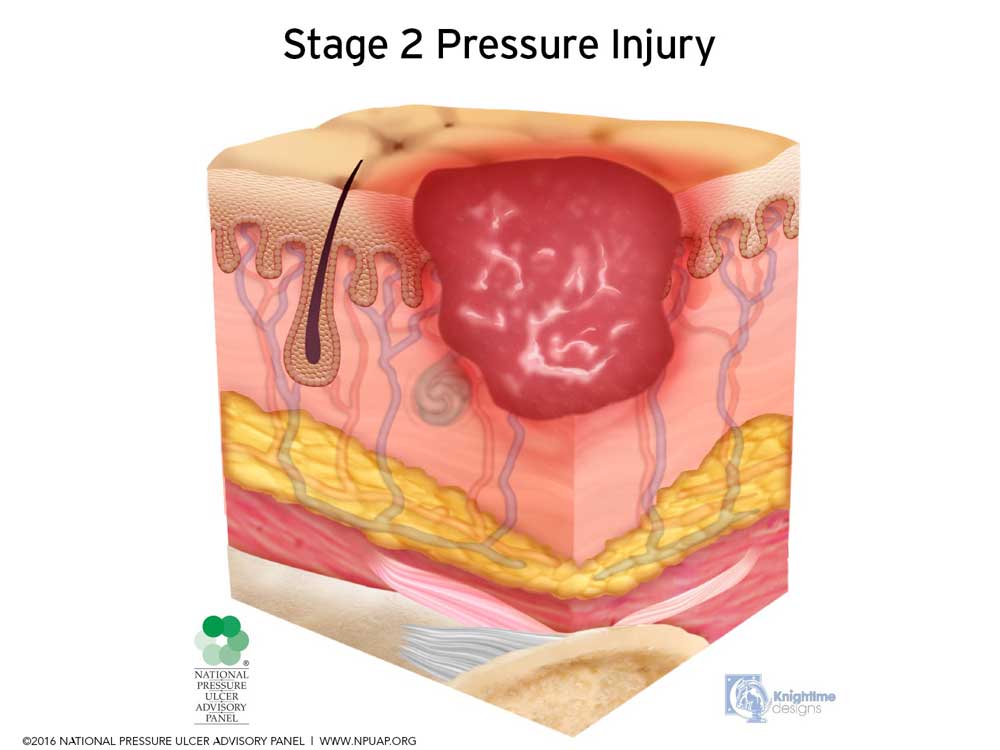
局部皮肤缺失并暴露部分真皮层。伤口床具有活性、呈粉色或红色、湿润,并且还表现为完整或破损的浆液性水疱。脂肪及深部组织不可见。无肉芽组织,腐肉和焦痂。这些损伤通常是由于骨盆上皮肤的微环境破坏和受到剪切力以及足跟的剪切力造成的。此阶段不应用于描述与潮湿相关的皮肤损伤(MASD),例如失禁相关性皮炎(IAD),皮肤皱褶处皮炎(ITD),医学粘合剂相关皮肤损伤(MARSI)或创伤性伤口(皮肤撕裂,烧伤,擦伤)。
第3阶段压力损伤:全层皮肤缺失
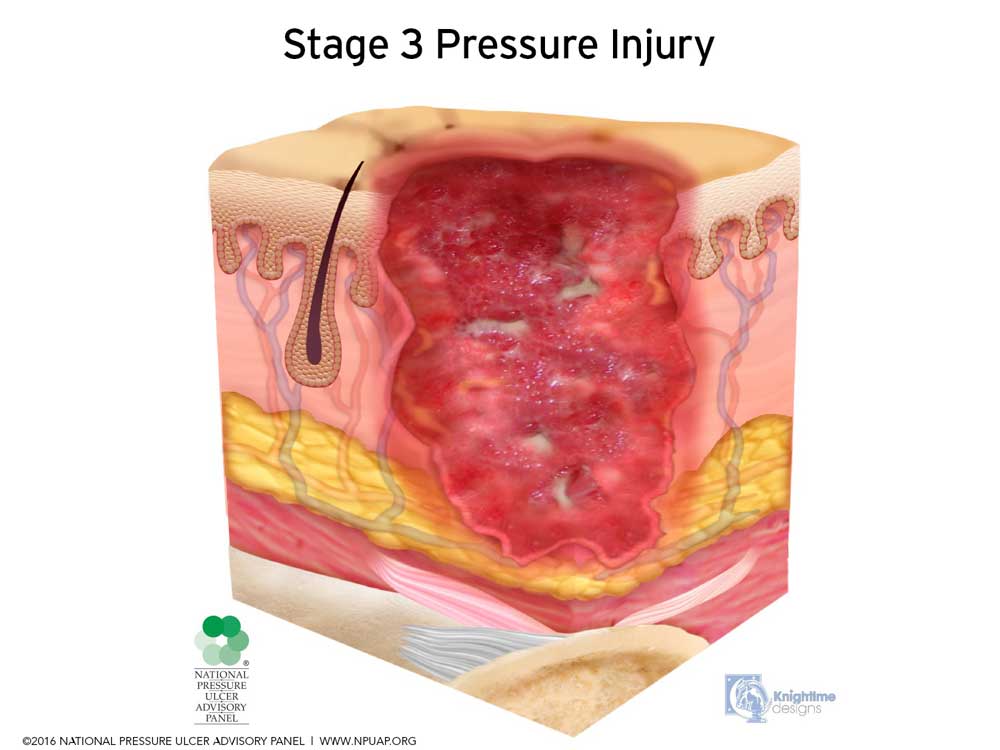
第3阶段压力损伤 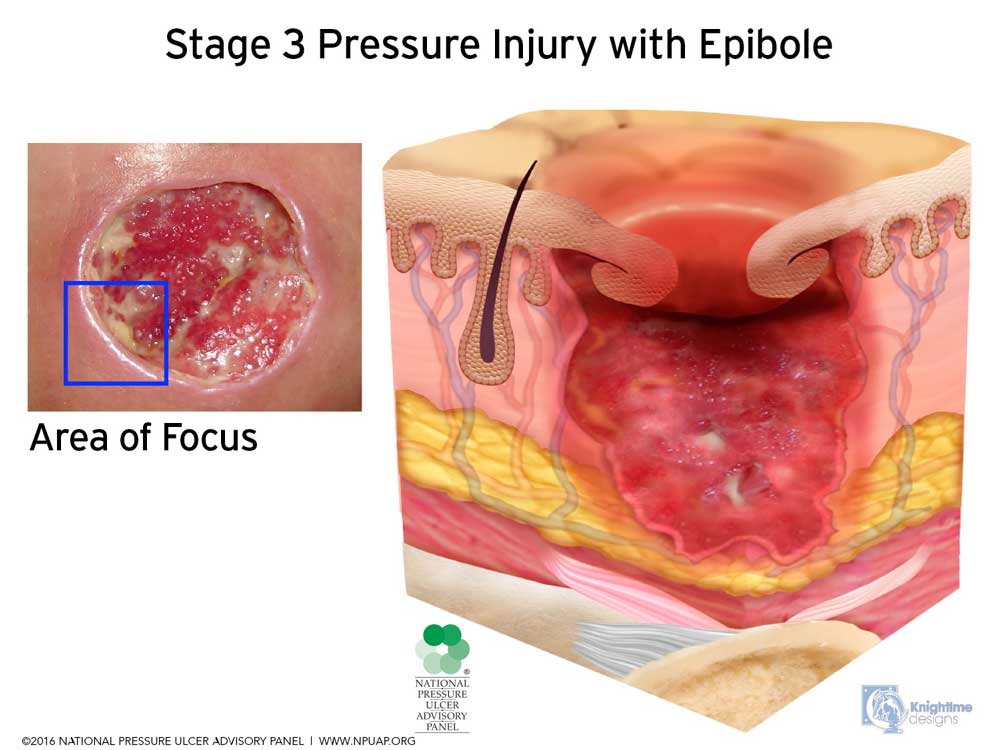
第3阶段压力损伤-卷边
全层皮肤缺失,通常存在可见脂肪、肉芽组织和皮肤边缘内卷。可见腐肉和/或焦痂。组织损伤的深度因解剖位置不同存在差异;脂肪丰富的区域会发展成深部伤口。可能会出现潜行或窦道。无筋膜,肌肉,肌腱,韧带,软骨和/或骨暴露。如果腐肉或焦痂掩盖组织缺损的深度,则这是一种不可划分阶段的压力损伤。
第4阶段压力损伤:全层皮肤和组织损失
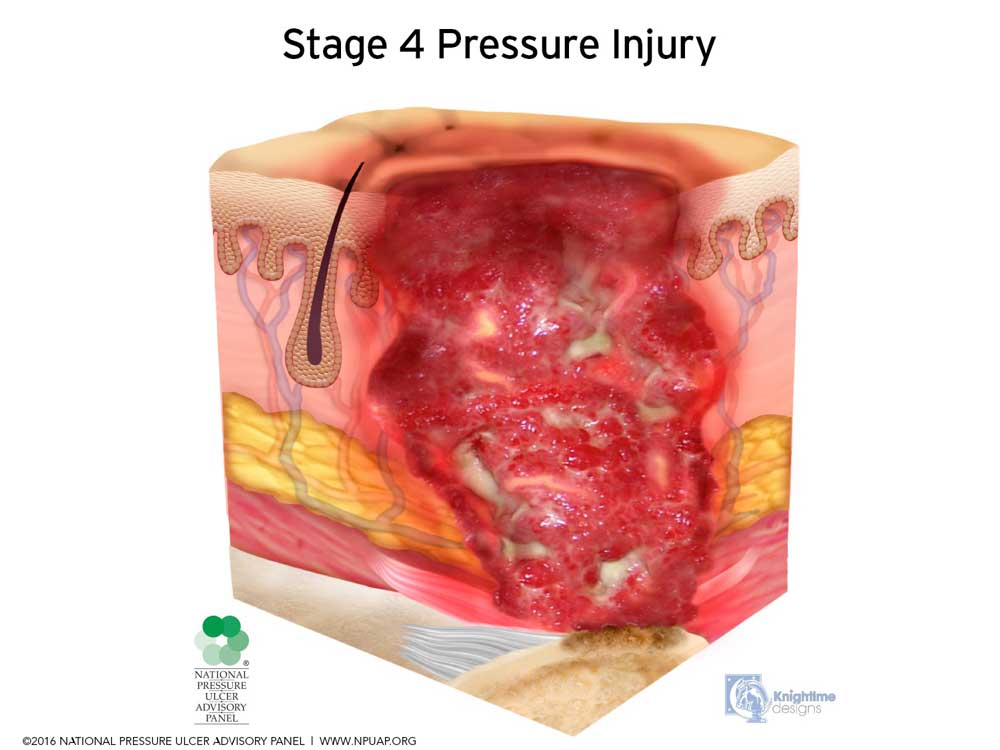
第4阶段压力损伤:全层皮肤和组织损失
溃疡中暴露或直接可触及到筋膜、肌肉、肌腱、韧带、软骨或骨头。可以看到腐肉和/或焦痂。经常发生Epibole(卷边),窦道和/或潜行效应。不同解剖位置的组织损伤的深度存在差异。如果腐肉或焦痂掩盖组织缺损的深度,则为不可划分阶段压力性损伤。
不可划分阶段压力损伤:全层皮肤和组织缺失,损伤程度被掩盖
深部组织压力损伤 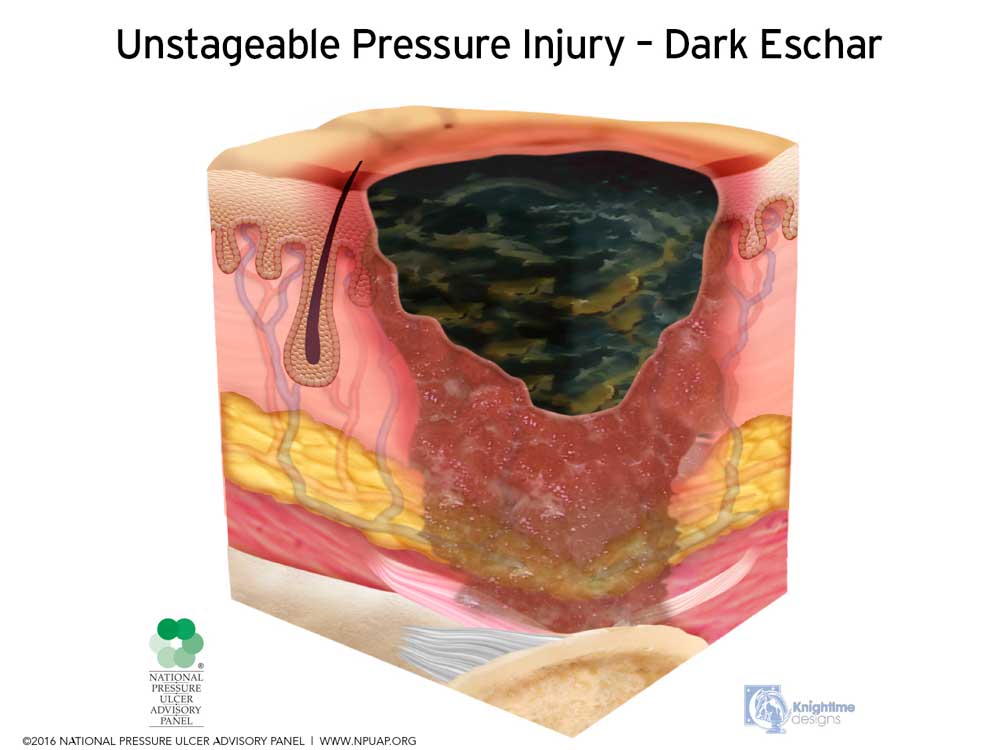
不可划分阶段压力损伤-焦痂 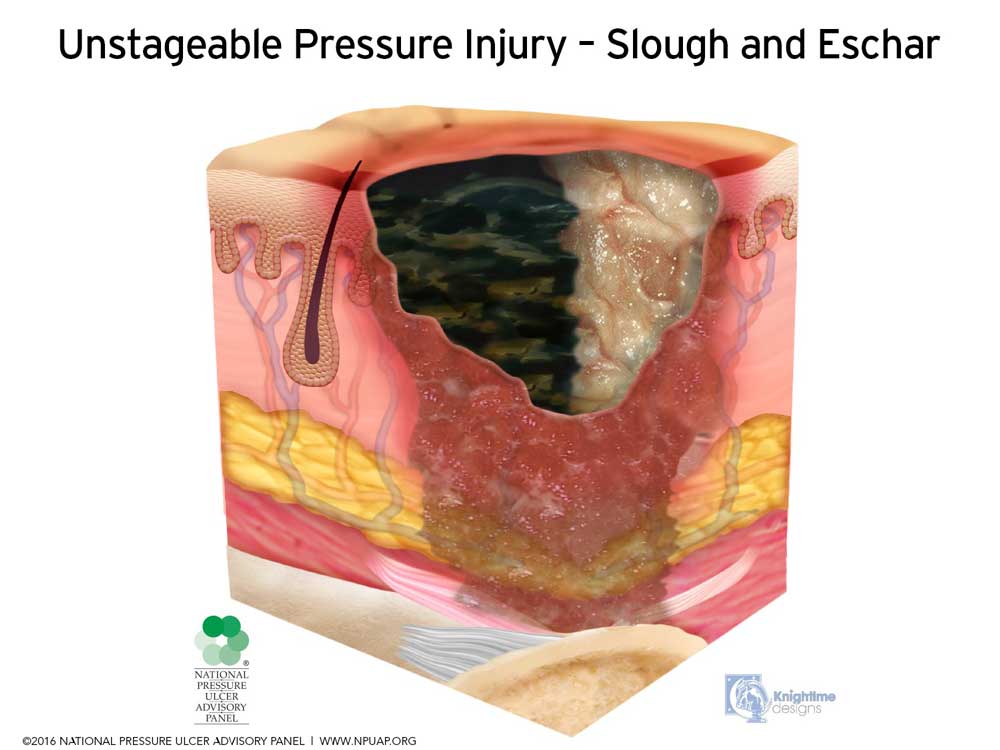
不可划分阶段压力损伤-腐肉和焦痂
全层皮肤和组织缺失,由于被腐肉和/焦痂掩盖,溃疡内的组织损伤程度无法确认。只有去除足够的腐肉和/或焦痂,才能判断损伤是第3阶段还是第4阶段。缺血肢端或足跟的稳定型焦痂(即为:干燥,紧密粘附,完整无红斑和波动感)不应软或化去除。
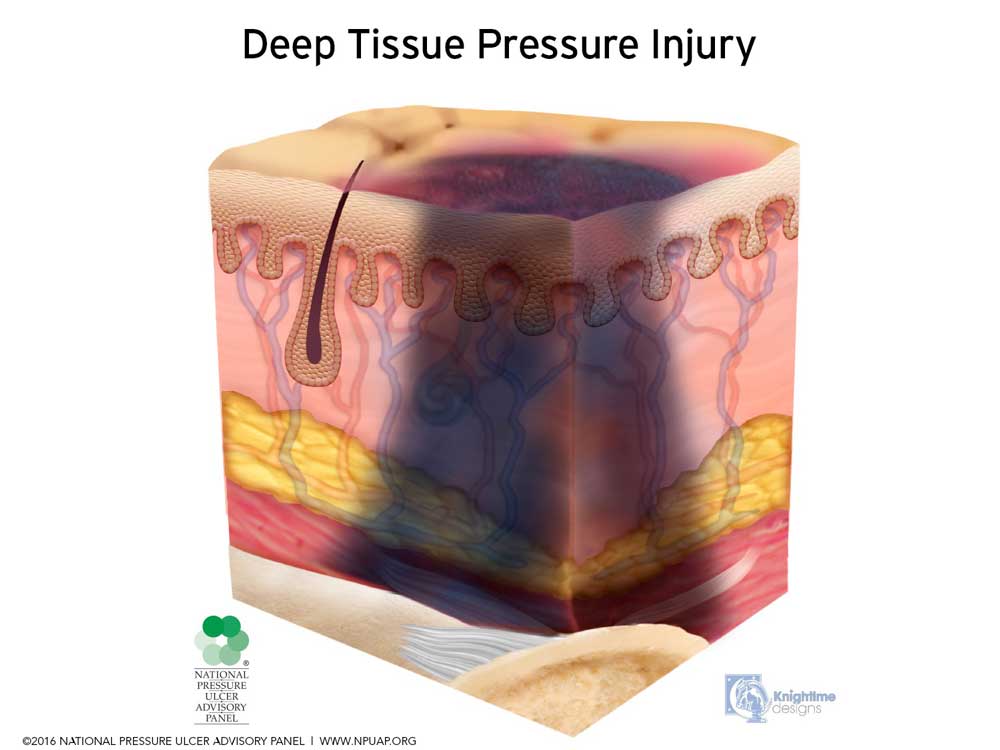
深部组织压力损伤:持续不可褪色的深红色,栗色或紫色变色
完整或破损的局部皮肤出现持续的指压不变白深红色,栗色或紫色,或表皮分离露出黑色的伤口床或充血水疱。疼痛和温度变化通常先于皮肤颜色变化出现。在深色皮肤中,变色可能会有所不同。这种损伤是由于强烈和/或长期的压力和剪切力作用于骨骼和肌肉交界面导致。伤口可迅速发展暴露组织缺失的实际程度,也可能溶解而不出现组织缺失。如果可见坏死组织、皮下组织、肉芽组织、筋膜、肌肉或其他深层结构,则表明这是全皮层的压力损伤(不可分阶段,第3阶段或第4阶段)。该阶段不可用于描述血管、创伤、神经性伤口或皮肤病。
附加的压力损伤定义:
医疗器械相关的压力损伤:
描述了损伤病因。
与医疗设备相关的压力损伤源于使用设计和应用于诊断或治疗目的的设备,所产生的压力损伤通常符合装置的图案或形状。损伤可以使用分阶段系统进行划分。
粘膜压力损伤:
在粘膜上发现粘膜压力损伤,并且在损伤部位有使用医疗器械的历史。由于损伤组织的解剖特点,这一类损伤无法进行分阶段。
[otw_shortcode_content_toggle title=”英文原文” opened=”closed” icon_type=”general foundicon-star”]
NPUAP Pressure Injury Stages
The National Pressure Ulcer Advisory Panel redefined the definition of a pressure injuries during the NPUAP 2016 Staging Consensus Conference that was held April 8-9, 2016 in Rosemont (Chicago), IL.
The updated staging definitions were presented at a meeting of over 400 professionals. Using a consensus format, Dr. Mikel Gray from the University of Virginia adeptly guided the Staging Task Force and meeting participants to consensus on the updated definitions through an interactive discussion and voting process. During the meeting, the participants also validated the new terminology using photographs.
The updated staging system includes the following definitions:
Pressure Injury:
A pressure injury is localized damage to the skin and underlying soft tissue usually over a bony prominence or related to a medical or other device. The injury can present as intact skin or an open ulcer and may be painful. The injury occurs as a result of intense and/or prolonged pressure or pressure in combination with shear. The tolerance of soft tissue for pressure and shear may also be affected by microclimate, nutrition, perfusion, co-morbidities and condition of the soft tissue.
Stage 1 Pressure Injury: Non-blanchable erythema of intact skin
Intact skin with a localized area of non-blanchable erythema, which may appear differently in darkly pigmented skin. Presence of blanchable erythema or changes in sensation, temperature, or firmness may precede visual changes. Color changes do not include purple or maroon discoloration; these may indicate deep tissue pressure injury.
Stage 2 Pressure Injury: Partial-thickness skin loss with exposed dermis
Partial-thickness loss of skin with exposed dermis. The wound bed is viable, pink or red, moist, and may also present as an intact or ruptured serum-filled blister. Adipose (fat) is not visible and deeper tissues are not visible. Granulation tissue, slough and eschar are not present. These injuries commonly result from adverse microclimate and shear in the skin over the pelvis and shear in the heel. This stage should not be used to describe moisture associated skin damage (MASD) including incontinence associated dermatitis (IAD), intertriginous dermatitis (ITD), medical adhesive related skin injury (MARSI), or traumatic wounds (skin tears, burns, abrasions).
Stage 3 Pressure Injury: Full-thickness skin loss
Full-thickness loss of skin, in which adipose (fat) is visible in the ulcer and granulation tissue and epibole (rolled wound edges) are often present. Slough and/or eschar may be visible. The depth of tissue damage varies by anatomical location; areas of significant adiposity can develop deep wounds. Undermining and tunneling may occur. Fascia, muscle, tendon, ligament, cartilage and/or bone are not exposed. If slough or eschar obscures the extent of tissue loss this is an Unstageable Pressure Injury.
Stage 4 Pressure Injury: Full-thickness skin and tissue loss
Full-thickness skin and tissue loss with exposed or directly palpable fascia, muscle, tendon, ligament, cartilage or bone in the ulcer. Slough and/or eschar may be visible. Epibole (rolled edges), undermining and/or tunneling often occur. Depth varies by anatomical location. If slough or eschar obscures the extent of tissue loss this is an Unstageable Pressure Injury.
Unstageable Pressure Injury: Obscured full-thickness skin and tissue loss
Full-thickness skin and tissue loss in which the extent of tissue damage within the ulcer cannot be confirmed because it is obscured by slough or eschar. If slough or eschar is removed, a Stage 3 or Stage 4 pressure injury will be revealed. Stable eschar (i.e. dry, adherent, intact without erythema or fluctuance) on the heel or ischemic limb should not be softened or removed.
Deep Tissue Pressure Injury: Persistent non-blanchable deep red, maroon or purple discoloration
Intact or non-intact skin with localized area of persistent non-blanchable deep red, maroon, purple discoloration or epidermal separation revealing a dark wound bed or blood filled blister. Pain and temperature change often precede skin color changes. Discoloration may appear differently in darkly pigmented skin. This injury results from intense and/or prolonged pressure and shear forces at the bone-muscle interface. The wound may evolve rapidly to reveal the actual extent of tissue injury, or may resolve without tissue loss. If necrotic tissue, subcutaneous tissue, granulation tissue, fascia, muscle or other underlying structures are visible, this indicates a full thickness pressure injury (Unstageable, Stage 3 or Stage 4). Do not use DTPI to describe vascular, traumatic, neuropathic, or dermatologic conditions.
Additional pressure injury definitions.
Medical Device Related Pressure Injury:
This describes an etiology.
Medical device related pressure injuries result from the use of devices designed and applied for diagnostic or therapeutic purposes. The resultant pressure injury generally conforms to the pattern or shape of the device. The injury should be staged using the staging system.
Mucosal Membrane Pressure Injury: Mucosal membrane pressure injury is found on mucous membranes with a history of a medical device in use at the location of the injury. Due to the anatomy of the tissue these ulcers cannot be staged.
[/otw_shortcode_content_toggle]
如果本文对您有帮助,欢迎使用左边赞赏~
¥赞赏
评论